Diagnosis and Treatment
-
 In Skin Cancer Medicine accurate diagnosis is crucial. Without the correct diagnosis it is impossible to offer the correct treatment. Failure to diagnose melanoma can lead to loss of life. Without an accurate diagnosis, patients may also undergo unnecessary treatment.
In Skin Cancer Medicine accurate diagnosis is crucial. Without the correct diagnosis it is impossible to offer the correct treatment. Failure to diagnose melanoma can lead to loss of life. Without an accurate diagnosis, patients may also undergo unnecessary treatment.The aim is to make as accurate a diagnosis as possible with visual inspection. However, the diagnosis of early melanoma and other skin cancers can be extremely challenging. Increasingly this is becoming a specialised area and there is now overwhelming evidence that doctors trained in a technique known as dermoscopy are able to diagnose melanoma and other skin cancers at an earlier stage.
Dermoscopy involves using an instrument known as a dermatoscope, often in combination with a liquid such as alcohol, to visualise the structures beneath the skin. Apart from improving skin cancer diagnosis it also improves the ability to confidently diagnose non malignant skin lesions and therefore reduces the number of unnecessary excisions.
However, even in the most skilled hands, it is not always possible to make a definite diagnosis by observation only. Sometimes it is necessary to take a biopsy (a sample of tissue) to confirm a diagnosis. Biopsies are often also useful because they give the treating doctor information about the type and behaviour of the skin cancer which can be valuable for planning further treatment.
There are two other techniques that can be utilised to assist in the diagnosis of early melanoma.
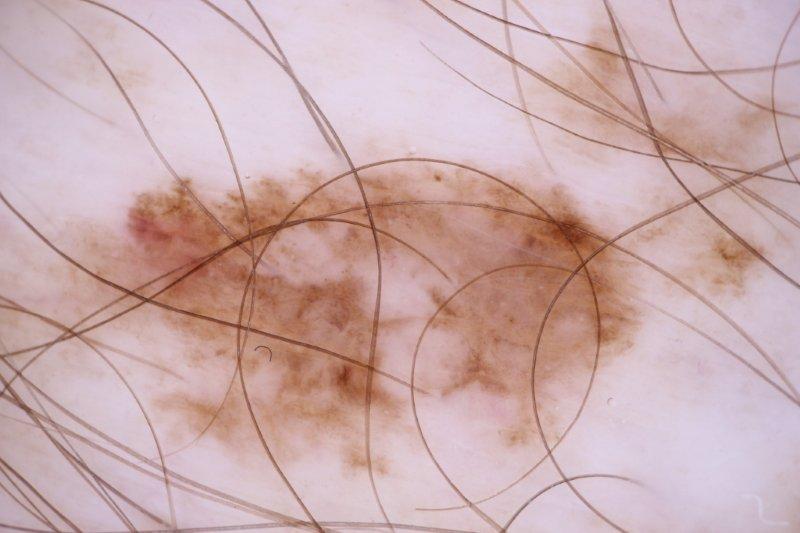
- Short term monitoring. If a mole is new or growing it has a higher chance of being malignant. Monitoring
involves photographing an individual mole and rephotographing it 3 months later. If the mole changes it is usually removed (even if it still doesn't exhibit features of melanoma). The melanoma below was detected by identifying change on short term monitoring. Click on images to enlarge.
- Total Body Photography. The main limitation of monitoring is that it only allows follow up of a limited number of moles that have been classified as potentially suspicious. If a mole that is an early melanoma is not monitored the chance for early detection will be lost. Total Body Photography involves taking a series of studio quality photographs of the entire skin surface. These images can be used by the Skin Cancer Clinic to look for new or changing moles. Most experts agree that this is the best early detection strategy for patients at high risk of melanoma. For more information, click here.
Even with all the knowledge and skill necessary, melanomas will be missed if they are not looked for. A proper skin examination requires a thorough inspection of all areas of the skin with a patient undressed to their underwear. This is generally not something that can be done in 10 minutes or less, especially for somebody that has a lot of moles or a history of skin cancer. More is missed by not looking than not knowing!
- Short term monitoring. If a mole is new or growing it has a higher chance of being malignant. Monitoring
-
 Surgery is considered the best treatment for the majority of skin cancers. One of the main advantages of surgery over other forms of treatment is that it allows the removed skin tissue to be examined by a pathologist. This helps confirm the diagnosis as well as completeness of removal.
Surgery is considered the best treatment for the majority of skin cancers. One of the main advantages of surgery over other forms of treatment is that it allows the removed skin tissue to be examined by a pathologist. This helps confirm the diagnosis as well as completeness of removal.It is important that when skin cancers are removed that there is a margin of normal healthy tissue around the skin cancer that is also removed. The size of the margin required depends on the type of skin cancer removed. It is wrong to try and minimise the length of the scar by compromising the size of the margin. Inadequate margins increase the risk of recurrence.
Surgery that is well planned and executed can give excellent cosmetic results. A variety of techniques can be used to give minimise scar formation. The insertion of internal dissolving sutures minimises tension in wounds and consistently leads to better cosmetic results. It takes considerable experience to insert this type of suture expertly. This technique is often utilised by Plastic Surgeons but experienced, well trained Skin cancer doctors also often utilise this technique.
Elliptical Excision
The majority of skin cancers are removed by a technique known as elliptical excision.
The following case illustrates a 72 year old gentleman with a squamous cell carcinoma on his lower leg.
Please click on the first image to follow the series of images demonstrating the various stages of surgery and wound healing.
As mentioned above, It is important that a margin of normal tissue be included beyond the area of visible skin cancer. This is to reduce the risk of incomplete excision or recurrence. Many doctors take inadequate margins when excising skin cancers.The following case illustrates a 73 year old lady with a basal cell carcinoma on her back.
Please click on the first image to follow the series of images demonstrating the various stages of surgery and wound healing.
Flap Closures
Sometimes it is necessary to close a surgical defect with what is known as a flap repair. This can be done in a variety of ways and usually involves either rotating or advancing skin from an adjacent area into the defect left after removing the skin cancer. Flaps are usually performed in order to maintain function or to enhance the cosmetic outcome eg. a direct elliptical closure near an eyebrow may cause a permanently elevated brow on one side. There has been criticism of some doctors working in Skin Cancer Clinics performing excessive numbers of flap procedures for financial gain.
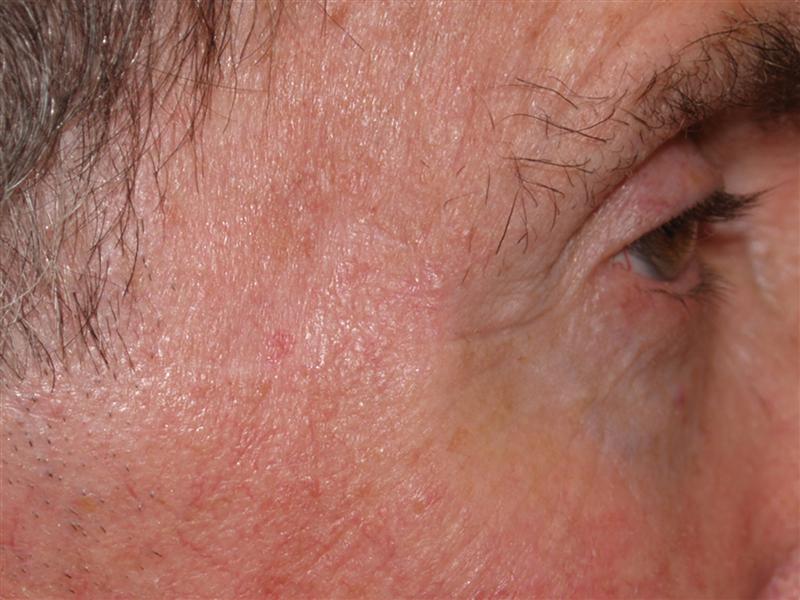
The following case illustrates a 66 year old gentleman with a basal cell carcinoma near his lower eyebrow. In this series of photographs, a technique known as a rhomboid flap has been used to close the defect following removal of a skin cancer on the temple. A flap was chosen to avoid the eyebrow being distorted by a direct closure.
Please click on the first image to follow the series of images demonstrating the various stages of surgery and wound healing.
-
Not all skin cancers have to be managed by surgical removal. It is not correct to think that surgery is necessarily a better treatment. All treatments have advantages and disadvantages. It is important that a Skin Cancer Doctor is able to discuss the various treatment option with each patient so that the best decision on treatment can be made for each individual.
Generally speaking non-surgical treatments are an option for patients with certain types of skin cancers that are confined to the surface layers of the skin. Precancerous sun spots are almost always treated non-surgically. Non-surgical treatments are usually not appropriate to treat melanoma.
Cryotherapy
 Cryotherapy involves using a very low temperatures to destroy abnormal or diseased skin tissue. Most commonly liquid nitrogen is used and sprayed in a precisely controlled manner onto the skin. Precancerous sunspots (actinic keratoses) are commonly treated in this way. Cryotherapy can also be used to treat superficial non-melanoma skin cancers but the spray needs to be applied for much longer and is therefore more painful and takes longer to heal.
Cryotherapy involves using a very low temperatures to destroy abnormal or diseased skin tissue. Most commonly liquid nitrogen is used and sprayed in a precisely controlled manner onto the skin. Precancerous sunspots (actinic keratoses) are commonly treated in this way. Cryotherapy can also be used to treat superficial non-melanoma skin cancers but the spray needs to be applied for much longer and is therefore more painful and takes longer to heal.Cryotherapy is quick and can be effective if used appropriately. Many people find it painful and the treated areas can blister, scab and ooze. In certain areas of the body such as the lower legs healing can take many weeks. Often areas that have been treated in this way heal with a permanent white scar.
Curettage and Cautery
Curettage
 and Cautery is a technique that involves scraping away cancerous or precancerous skin with a sharp circular instrument known as a curette. The area is then cauterised with either a hot wire beaded tip or an electrosurgical unit. This helps stop bleeding and helps remove any remaining abnormal skin. Often the process is repeated 2 or 3 times.
and Cautery is a technique that involves scraping away cancerous or precancerous skin with a sharp circular instrument known as a curette. The area is then cauterised with either a hot wire beaded tip or an electrosurgical unit. This helps stop bleeding and helps remove any remaining abnormal skin. Often the process is repeated 2 or 3 times.Curettage and cautery is often used to treat patients with multiple small, well defined non-melanoma skin cancers. It is not a suitable treatment for melanoma. Skin cancers that are large, deep or recurrent are also not suitable for this technique.
Curettage and cautery is relatively quick and easy to perform. However, the areas treated often have pale, round scars. These scars are usually about the same size as the skin cancer being treated. Areas treated on the lower legs can take many weeks to heal.
Topical Creams
Creams can be used to treat precancerous sunspots and, in certain circumstances, superficial non-melanoma skin cancers. They are not suitable to treat melanoma.
There are three creams available in Australia:
Aldara
Aldara can be used to treat precancerous sunspots and certain types of superficial skin cancer (especially superficial basal cell carcinoma). It is generally used 3 to 5 times per week for up to 6 weeks depending on the condition being treated. The treated area can become red, inflamed, tender and scabbed. Sometimes patients report flu-like symptoms when using this cream. Cure rates are around 80%.
Efudix
This cream has been used for decades as a treatment for precancerous sunspots and, less frequently, certain surface skin cancers. When used for sunspots it tends to cause a very brisk, intense reaction that some patients find difficult to tolerate. It is generally used twice daily for 2 to 4 weeks. There is a newer cream called Tolak which is similar to efudix but only has to be used once daily.
Efudix / Calcipotriol
This is a relatively new treatment for precancerous sunspots. It is compounded by a pharmacy by adding standard efudix cream to calcipotriol (Vitamin D cream). The advantage of this approach is that the length of treatment is considerably shorter ie. 4 to 7 days for the face and 7 to 10 days for other areas.
A word of warning .........
There is a cream being marketed as "black salve" or "cansema". This cream is potentially very dangerous. It causes indiscriminate destruction of skin tissue and can lead to permanent disfiguring scarring. Never use any cream on a suspected skin cancer without consulting your GP or an experienced Skin cancer Doctor.