Types of Skin Cancer
Skin cancer – what to look for
There are three common skin cancers – basal cell carcinomas (BCC), squamous cell carcinomas, (SCC) and melanoma. BCCs and SCCs constitute the bulk of “non-melanoma skin cancer” (NMSC), of which there are around 430,000 treated each year in Australia. There are over 18,000 melanomas diagnosed in Australia each year of which around 1,500 prove to be fatal.
-
Basal cell carcinoma is also known as BCC it is the commonest cancer in the world. It is estimated that two out of every three Australians will develop a BCC. Fortunately, very few people actually die from this type of skin cancer. This is because it does not spread through the body and invade other organs. It tends to grow slowly, often as a small nodule or a non-healing sore. Eventually they ulcerate and can start growing into the surrounding skin. If left long enough they can grow deeply and be very disfiguring.
There are different types of BCC.
- Superficial and nodular BCC are the most common and least aggressive. They tend to grow relatively slowly in the upper parts of the skin. They are usually fairly easily treated and cured by surgical treatment or, in some cases, non-surgical methods.
- More aggressive types of BCC include infiltrative, morphoeic and micro-nodular varieties. These tend to grow deeper and wider and are often difficult to diagnose. These types often require more aggressive surgical treatment. More aggressive types of BCC can travel down nerves and cartilage and enter the skull if not adequately treated; these aggressive BCCs are often the most difficult to recognise.
Causes for BCCs
BCCs are most commonly caused by fair skin individuals with significant exposure to the sun rays during early years of life, usually before the age of 10. Intermittent, blistering or peeling sunburn is thought to lead to the formation of BCCs.
Other causes are rare such as certain genetic errors or carcinogen exposure (e.g. arsenic ingestion).
There is limited evidence that the use of sunscreen prevents the development of BCC – only sun avoidance and protective clothing will be effective.
How are BCCs Diagnosed?
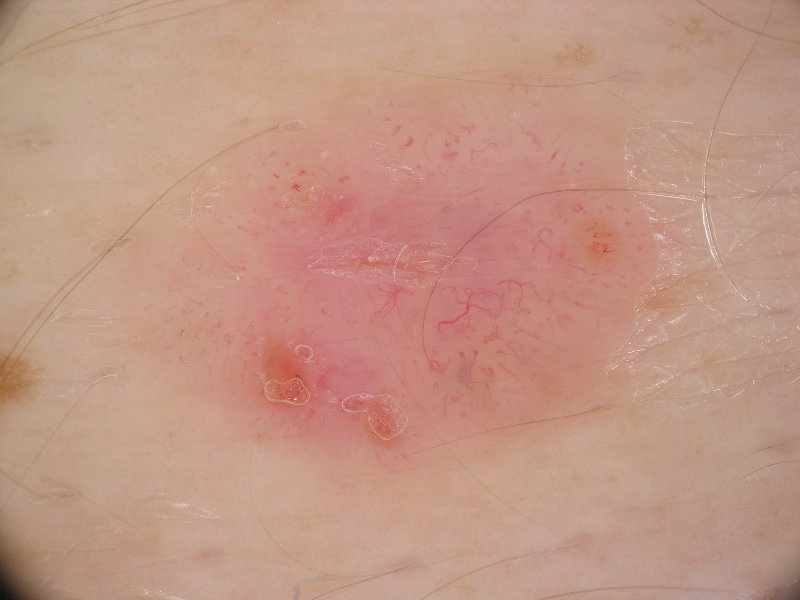
BCCs are usually diagnosed by visual inspection. Some doctors use good lighting with magnification but dermoscopy is the best technique for diagnosing small and subtle BCCs. This technique allows the identification of a whole range of features below the surface of the skin not visible to the naked eye.
The following photographs are taken by attaching a digital camera to a dermatoscope.
Please click on the images to enlarge them.
Treatment options
It is very important to avoid excessive sun-exposure in early life. However, BCCs are easily curable if treatment is early, depending on the type and site of the cancer. Treatment options are:
- Surgical Excision - usually the best option
- Curettage and cautery - a technique of scraping and burning the lesion, useful for superficial BCCs
- Topical creams such as Aldara for 6 weeks – only for superficial BCCs
- Radiotherapy for some advanced cases where surgery cannot guarantee complete cure
-
Squamous Cell Carcinoma (SCC) is the second commonest skin cancer. They tend to grow faster than BCCs and are potentially more dangerous as they can spread to other parts of the body. SCCs on the scalp, lip and ear have the tendancy to behave aggressively and are at increased risk of spreading. About 300 people die each year in Australia from SCC.
Sun-spots (actinic keratosis or solar keratosis) are actually SCCs in their earliest form. These spots are generally not classified as skin cancers but rather as precancerous. Only a very small percentage of sun-spots ever become SCCs but it is thought that most SCC’s do start out as a sun-spot, hence sun-spots should be treated. When a sun-spot become a SCC, it usually stings or becomes sore and then grows fairly quickly.
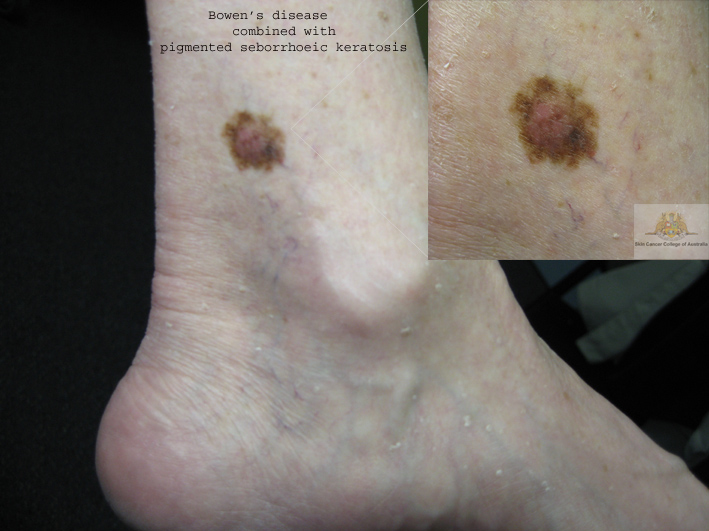
Bowen's Disease is another form of pre-invasive SCC. It is classified as a type of skin cancer but does not have the potential to spread to other parts of the body unless it becomes invasive. Bowen's Disease often occurs on the lower legs and can often be treated non-surgically.
Keratoacanthoma is a rapidly growing SCC like tumour. It is benign but nevertheless can be very destructive. Keratoacanthoma often resolves by itself.
Pictures of Solar Kertosis (Click to enlarge)
Causes for SCCs
The vast majority of SCCs are due to chronic exposure of fair skinned individual UV light. SCC is generally caused by cumulative or total sun exposure rather than intermittent burning and peeling. Therefore it is particularly prevalent in outdoor workers.
Other causes are smoking (particularly important for lip/mouth/tongue cancers), scars, chronic leg ulcers, organ transplant immunosuppressive drugs and infection with human papilloma virus.
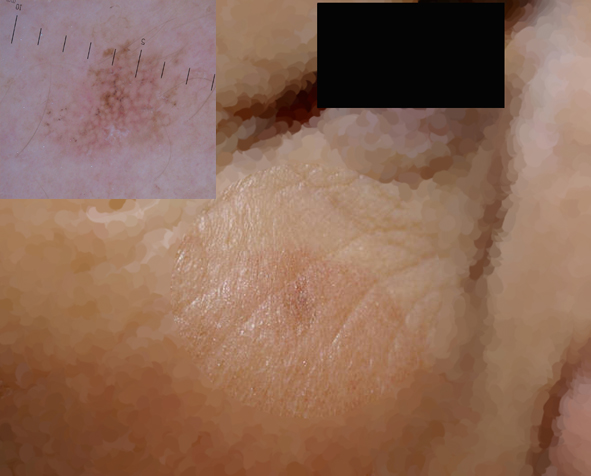
How is SCC Diagnosed?
SCC is diagnosed clinically ie. by taking a history and by visual inspection. Dermoscopy is useful as an adjunct for diagnosing SCC. Dermoscopy can also be used to help decide which sun-spots are more likely to turn into invasive SCC. Dermoscopy is invaluable in diagnosing Bowen's Disease.
Pictures of SCC (click to enlarge)
Treatment options
SCCs are easily curable if treatment is early. Treatment options are:
- Excision – usually the best option
- Freezing with liquid nitrogen is effective for well defined single sunspots
- Topical creams such as Efudix, Aladara, Tolak and compounded Efudix/Calcipotriol cream can be used for sun-spots
- Curettage and cautery - a technique of scraping and burning the lesion, useful for superficial SCCs
- Radiotherapy for some advanced cases where surgery cannot guarantee complete cure
Sun-screen does have a role in preventing and promoting regression of SCCs and sun-spots
-
Melanoma is lethal
 Melanoma is one of the deadliest cancers. It has the potential to spread into the body and appear in the lymph nodes, liver, brain, bones, lungs and other parts of the body. The chance of cure depends entirely on the stage at which the melanoma is diagnosed.
Melanoma is one of the deadliest cancers. It has the potential to spread into the body and appear in the lymph nodes, liver, brain, bones, lungs and other parts of the body. The chance of cure depends entirely on the stage at which the melanoma is diagnosed. - Patients with melanomas that are diagnosed in the earliest stages before they have grown down into the skin have a survival rate of 100%.
- Patients with melanomas less than 1mm thick at diagnosis have a survival rate of over 95%.
- Patients with melanomas over 4mm thick at diagnosis have a survival rate of less than 50%.
The melanoma on the right was over 4mm deep at diagnosis. The patient subsequently died.
Melanoma is Common
Australia has the highest rate of melanoma in the world. About one in 15 Australian men will develop melanoma and about one in 24 Australian women will develop melanoma. In 2008 there were 1430 deaths in Australia from melanoma.
Melanoma is the most common cancer in people aged 15 - 44 years.
The situation is even worse on the Central Coast of NSW. The incidence of melanoma on the Central Coast is significantly higher than the NSW average for both men and women. Per capita, melanoma is about 25% more common on the Central Coast.
Risk factors for development of melanoma
- The most important risk factor in Australia is excessive exposure to natural sun light in fair skinned individuals.
- Intense, intermittent sun exposure causing blistering or peeling is associated with increased risk of melanoma.
- Other common risk factors are: large number of moles, especially irregular shaped moles, large birth marks and family history of melanoma
Types of melanoma
- Superficial spreading melanoma is most common type and most amendable to simple excision.
- Nodular melanoma is the most dangerous melanoma as they are often very thick when diagnosed
- Lentigo maligna melanoma is most commonly found in elderly patients usually on the face or neck
- Melanoma in situ is the earliest form of melanoma and is totally curable with complete excision.
- Acral melanoma is on the sole of the foot or on the palm of the hand – it is uncommon and often goes unnoticed
Treatment options
It is very important to avoid excessive sun-exposure in early life and, remember sun-screen may not prevent development of melanoma so wearing protective clothing is your most important insurance against this disease.
Melanomas are curable in the majority if diagnosed and treated early. The gold standard of treatment for melanoma is complete excision, with a border of normal skin included in the excision: 5mm margin for in situ melanoma and 1.00 – 2.00 cm for more advanced melanoma.
How is Melanoma Diagnosed?
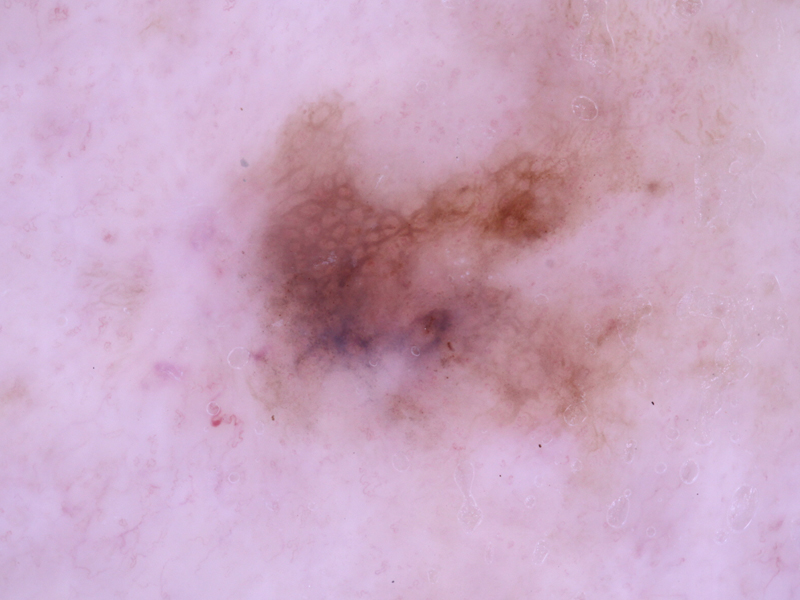
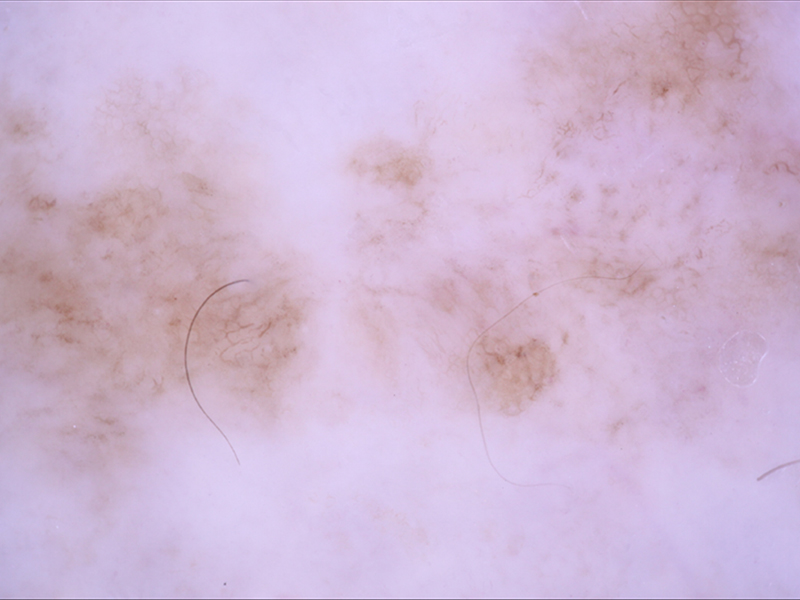
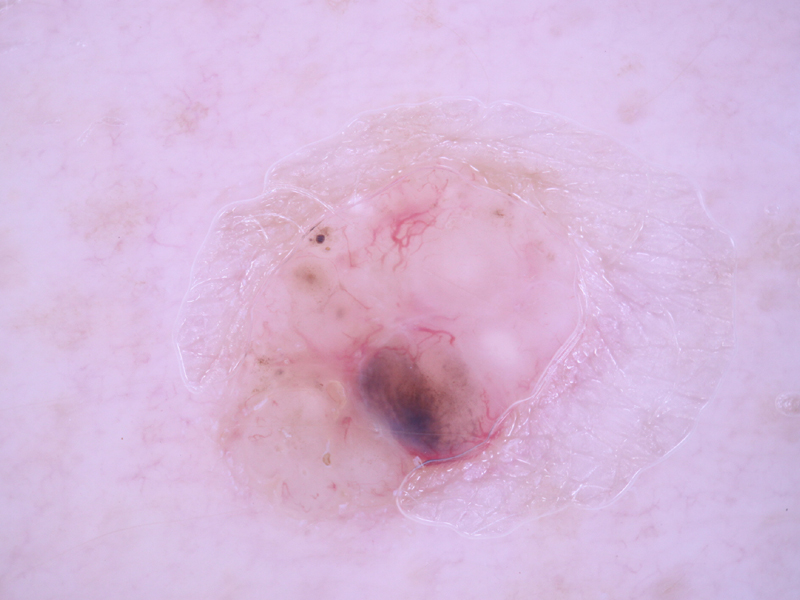
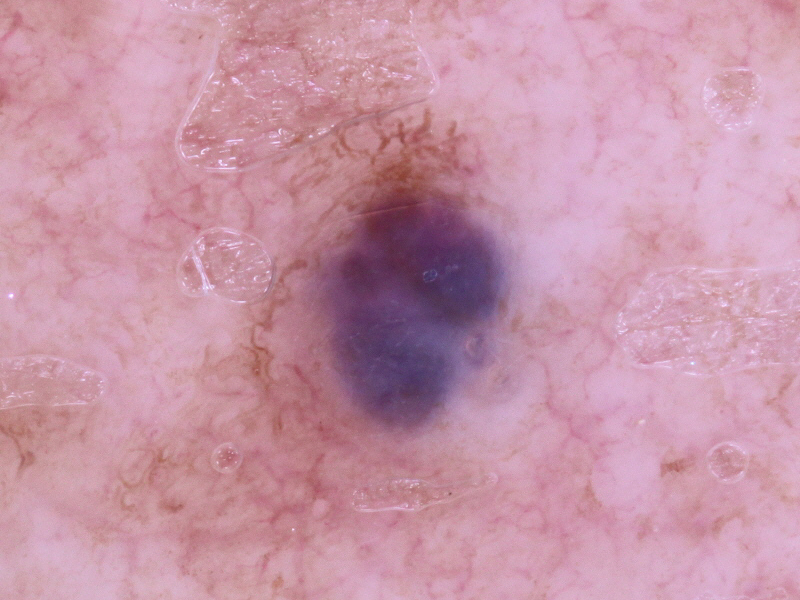
It is now generally regarded that a technique known as dermoscopy allows the clinician to diagnose melanoma at its earliest stages and also helps reduce the number of unnecessary excisions. The following photographs are all taken at Skin Integrity. The photographs have been taken by attaching a digital camera to the dermatoscope.
Please click on the images to enlarge them.
As you can see, there is a vast variety of presentations for melanoma. It is imperative that you receive a skin cancer examination from somebody that is adequately trained with dermoscopy.
Benign lesions which may look like melanoma
- Seborrheic keratosis - very common and often called an age-wart, senile wart or greasy wart
- Solar lentigo - flat brown lesion and known as liver spot or age spots – these are related to the seborrheic keratosis
- Haemangioma - a small blood blister-like lesion which is reddish or purple; there are usually quite a few present and can be a nuisance when nicked by the razor during shaving – they bleeds profusely!













.jpg)